What is a Submassive pulmonary embolism
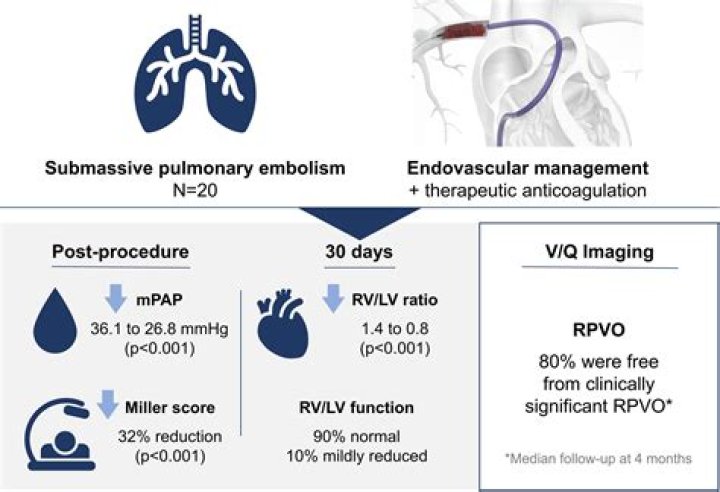
Submassive (or intermediate-risk) PE refers to those patients with acute PE without systemic hypotension but with evidence of either right ventricle (RV) dysfunction or myocardial necrosis.
What is the difference between massive and Submassive PE?
High-risk submassive PE: Hemodynamically stable patients who nonetheless have elevated mortality. They merit ICU admission and consideration for advanced therapies. Non-crashing massive PE: Patients with hypotension who stabilize well on low-dose vasopressor. These patients need ICU admission and advanced therapies.
How do you treat a Submassive PE?
The US Food and Drug Administration has approved tPA 100 mg administered as a continuous intravenous infusion over a 2-hour period for treatment of acute massive PE. Nevertheless, tPA is often used off-label to treat submassive PE.
What does Submassive mean?
(sŭb″mas′iv) [ sub- + massive] Medical jargon for very severe or injurious but not immediately life-threatening conditions. It is applied to diseases such as liver necrosis (without fulminant hepatic failure) or pulmonary embolism (without unstable hemodynamics).What is Submassive saddle PE?
2 Submassive PE is defined by evidence of right ventricular dysfunction with hemodynamic stability. 2 Although massive PEs are rare and comprise only about 2–5% of all PEs,3–5 they are crucially important because they carry a 52.4% 90-day mortality rate.
How is massive pulmonary embolism diagnosed?
Massive pulmonary embolism (PE) is characterized by systemic hypotension (defined as a systolic arterial pressure < 90 mm Hg or a drop in systolic arterial pressure of at least 40 mm Hg for at least 15 min which is not caused by new onset arrhythmias) or shock (manifested by evidence of tissue hypoperfusion and hypoxia …
What are the odds of surviving a pulmonary embolism?
However, reported survival after venous thromboembolism varies widely, with “short-term” survival ranging from 95% to 97% for deep vein thrombosis8,9 and from 77% to 94% for pulmonary embolism,4,6,8,9 while “long-term” survival ranges from 61% to 75% for both deep vein thrombosis and pulmonary embolism.
How often are pulmonary embolisms asymptomatic?
This dilemma is illustrated in the recent data from the French Registry of venous thromboembolic diseases that includes 387 patients with PE. 23 In symptomatic patients, 87% had dyspnea, a prevalence similar to that noted in previous studies (Table 1); however, 34% of patients were asymptomatic.What causes massive pulmonary embolism?
In most cases, pulmonary embolism is caused by blood clots that travel to the lungs from deep veins in the legs or, rarely, from veins in other parts of the body (deep vein thrombosis). Because the clots block blood flow to the lungs, pulmonary embolism can be life-threatening.
What are the different types of pulmonary embolism?Based on location of the clot into pulmonary artery following terms are used A) saddle PE (large clot into main pulmonary artery), B) lobar PE (into big branch of pulmonary artery), or C) distal PE (into small branches of pulmonary artery).
Article first time published onWhat is low risk pulmonary embolism?
Abstract. Patients with pulmonary embolism (PE) can be stratified into two different prognostic categories, based on the presence or absence of shock or sustained arterial hypotension. Some patients with normotensive PE have a low risk of early mortality, defined as <1% at 30 days or during hospital stay.
What is catheter directed thrombolysis?
Catheter-directed thrombolysis is a minimally invasive treatment that dissolves abnormal blood clots in blood vessels to help improve blood flow and prevent damage to tissues and organs.
When is alteplase used?
Alteplase injection is used to dissolve blood clots that have formed in the blood vessels. It is used immediately after symptoms of a heart attack occur to improve patient survival. It is also used after symptoms of a stroke and to treat blood clots in the lungs (pulmonary embolism).
What is the average size of a pulmonary embolism?
The average number of PE per patient was 3.7 (maximum 12, minimum 1). Their average length was 2.7 cm. Nine patients had saddle emboli (9%), and 71% of emboli were at or below the MPAb.
How long does it take for a saddle PE to dissolve?
A DVT or pulmonary embolism can take weeks or months to totally dissolve. Even a surface clot, which is a very minor issue, can take weeks to go away. If you have a DVT or pulmonary embolism, you typically get more and more relief as the clot gets smaller.
Can you cough up a PE blood clot?
Symptoms of pulmonary embolism vary, depending on the severity of the clot. Although most people with a pulmonary embolism experience symptoms, some will not. The first signs are usually shortness of breath and chest pains that get worse if you exert yourself. You may cough up bloody sputum.
How long do you stay in the hospital for pulmonary embolism?
Many people who have a PE spend some time in the hospital to receive treatment. The length of this stay can depend on the severity of the PE. One study from 2008 found that the median length of hospital stay for a PE was 6 days. In some cases, it may be possible to receive treatment at home.
How long before a pulmonary embolism becomes fatal?
The most risky time for complications or death is in the first few hours after the embolism occurs. Also, there is a high risk of another PE occurring within six weeks of the first one. This is why treatment is needed immediately and is continued for about three months.
Is death by pulmonary embolism painful?
A pulmonary embolism is a blood clot that typically starts in the deep veins in the legs or arms. This blood clot can break free and travel through the body towards the lungs. Once the clot reaches the lungs, the patient can experience extreme chest pain with a high chance of cardiac arrest.
What are the warning signs of a pulmonary embolism?
- Shortness of breath.
- Chest pain that may become worse when breathing in.
- Cough, which may contain blood.
- Leg pain or swelling.
- Pain in your back.
- Excessive sweating.
- Lightheadedness, dizziness or passing out.
- Blueish lips or nails.
What is not one of the symptoms of a pulmonary embolism?
Half the people who have pulmonary embolism have no symptoms. If you do have symptoms, they can include shortness of breath, chest pain or coughing up blood. Symptoms of a blood clot include warmth, swelling, pain, tenderness and redness of the leg.
Who is most at risk for pulmonary embolism?
- Have been inactive or immobile for long periods of time.
- Have certain inherited conditions, such as blood clotting disorders or factor V Leiden.
- Are having surgery or have broken a bone (the risk is higher weeks following a surgery or injury).
Can you recover from pulmonary embolism?
Recovery from pulmonary embolism can vary based on the severity of the condition and the treatment. If NYU Langone doctors have treated you with medication only, for instance, you may recover rapidly. It may take months, however, for people who’ve had open surgery to regain their strength.
Can a PE be silent?
Although between 60% and 80% of pulmonary emboli are clinically silent, patients may report a variety of symptoms (TABLE 3), including cough, chest pain, chest tightness, shortness of breath (dyspnea), palpitation, or coughing up blood (hemoptysis); patients may present with tachypnea, tachycardia, and diaphoresis.
Should Subsegmental PE treated?
Guidelines on Treatment of Subsegmental PE A leading specialty society advises that patients with subsegmental PE without deep venous thrombosis receive anticoagulation if the risk of recurrence is high, and surveillance if recurrence risk is low.
What would happen if the left pulmonary artery was blocked by a blood clot?
The clot blocks the normal flow of blood. This blockage can cause serious problems, like damage to your lungs and low oxygen levels in your blood. The lack of oxygen can harm other organs in your body, too. If the clot is big or the artery is clogged by many smaller clots, a pulmonary embolism can be deadly.
What is the most useful laboratory test for determining a patient's prognostic risk when a PE is suspected or confirmed?
Computed tomography angiography (CTA) is the initial imaging modality of choice for stable patients with suspected pulmonary embolism. The American College of Radiology (ACR) considers chest CTA to be the current standard of care for the detection of pulmonary embolism.
What is Virchow's triad?
The three factors of Virchow’s triad include intravascular vessel wall damage, stasis of flow, and the presence of a hypercoagulable state.
What is risk stratification?
Risk Stratification. • Risk Stratification is defined as a ongoing process of assigning. all patients in a practice a particular risk status – risk status is. based on data reflecting vital health indicators, lifestyle and. medical history of your adult or pediatric populations.
When should thrombolysis be administered?
Ideally, you should receive thrombolytic medicines within the first 30 minutes after arriving at the hospital for treatment. A blood clot can block the arteries to the heart. This can cause a heart attack, when part of the heart muscle dies due to a lack of oxygen being delivered by the blood.
When is a catheter-directed thrombolysis used?
Catheter-directed thrombolysis can be used to treat DVTs as an adjunct to medical therapy. Appropriate indications include younger individuals with acute proximal thromboses, a long life expectancy, and few comorbidities or limb-threatening thromboses.