What is the difference between a physiologic S3 and a pathologic S3?
What is the difference between a physiologic S3 and a pathologic S3?
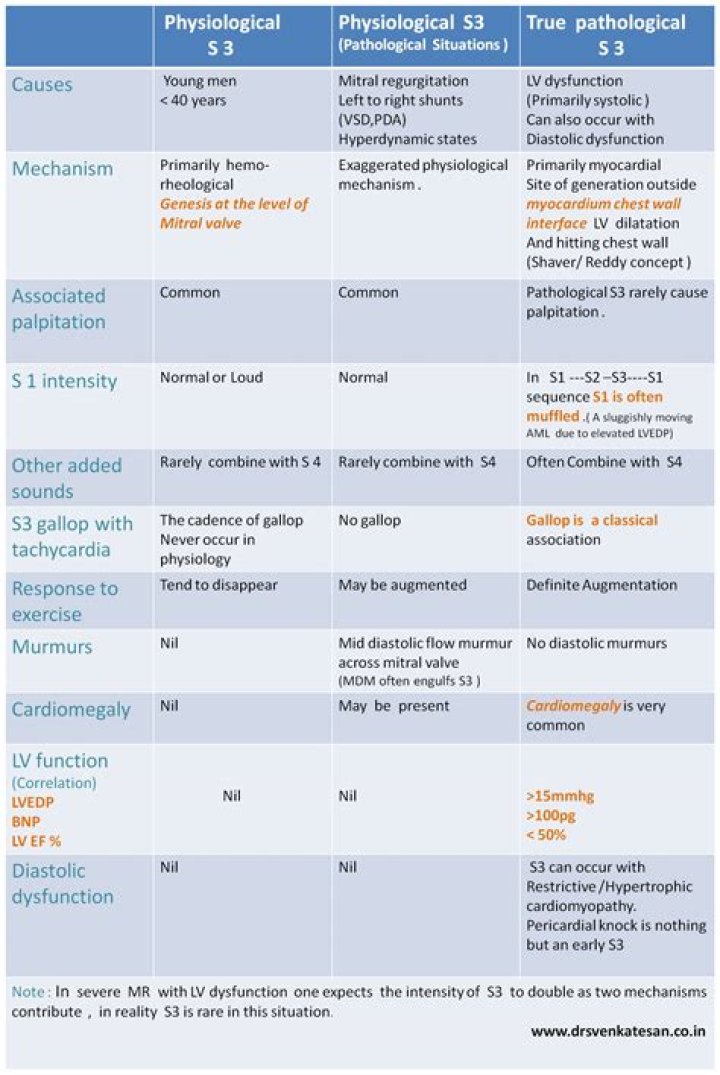
The S3 may be normal (physiological) or abnormal (pathological). The normal S3 usually disappears when the person sits up. In adults, the S¬3 is usually abnormal. The pathological S3 is also called a ventricular gallop or an S3 gallop, and it persists when sitting up.
What conditions decrease the intensity of s1?
Conditions associated with diminished intensity of S1 include the following: Inappropriate apposition of the AV valves (ie, mitral regurgitation [MR], tricuspid regurgitation [TR], dilated cardiomyopathy) Prolonged PR interval (ie, bradycardia, heart block, digitalis toxicity)
What is a normal cardiovascular assessment?
Documentation of a basic, normal heart exam should look something along the lines of the following: The external chest is normal in appearance without lifts, heaves, or thrills. PMI is not visible and is palpated in the 5th intercostal space at the midclavicular line. Heart rate and rhythm are normal.
What is the importance of assessing the heart and neck vessels?
Assessment of The Neck Vessels: Inspection The most important observation to be made in the neck region is the assessment of jugular venous pulse. From the jugular veins you can estimate central venous pressure (CVP) and estimate the heart’s efficiency as a pump.
What is the correct position of the client when assessing the heart and neck vessels?
The internal jugular veins provide information about blood volume and pressure in the right side of the heart. To measure the jugular venous pulse, position patient on his back and elevate the head of the bed 30 to 45 degrees, with the patient’s head turned slightly away from you.
How is a cardiovascular assessment performed?
The cardiac examination consists of evaluation of (1) the carotid arterial pulse and auscultation for carotid bruits; (2) the jugular venous pulse and auscultation for cervical venous hums; (3) the precordial impulses and palpation for heart sounds and murmurs; and (4) auscultation of the heart.
What are the 7 most important questions for cardiac medical history?
The most common and most important cardiac symptoms and history are: Chest pain, tightness or discomfort….Associated cough:
- Duration, paroxysms or constant, dry or productive?
- Associations: is it related to chest pains; any fever or shivering fits?
- Sputum: colour, quantity and any haemoptysis?
What should I ask for a cardiac assessment?
You will also want to ask about the patient’s history of heart disease, when and how it was treated, last EKG, stress tests, and serum cholesterol levels. Ask the patient the reasons for any previous hospitalizations and the nature of the treatments received while in the hospital.